
.png)
The NHS 10 Year Health Plan set out a clear direction of travel for the future of healthcare: bringing care closer to communities, focusing on prevention, and making a shift to digital. The Neighbourhood Health Framework (NHF) is the NHS’s attempt to operationalise that vision. It moves the conversation from strategy to implementation, setting out how neighbourhood-based, integrated care could work in practice.
As PUBLIC has seen first hand through our Health Innovation work with Thames Freeport, the key question is no longer whether neighbourhood health is the right model, but whether the system has the operational foundations, relationships, and infrastructure needed to make it work at scale.
The NHF represents a major shift in how the NHS organises and delivers care. At a high level, the Framework can be broken down into five national goals, three contracting models, and three directional shifts.
Together, these goals set the direction for a more preventative and locally-responsive health system. They identify the cohorts most likely to benefit from earlier intervention, support the shift of care away from hospitals, and reinforce the case for flexible, place-based delivery models that reflect the realities of local communities.
To support delivery, the NHF introduces three new contracting structures sitting beneath Integrated Care Boards (ICBs):
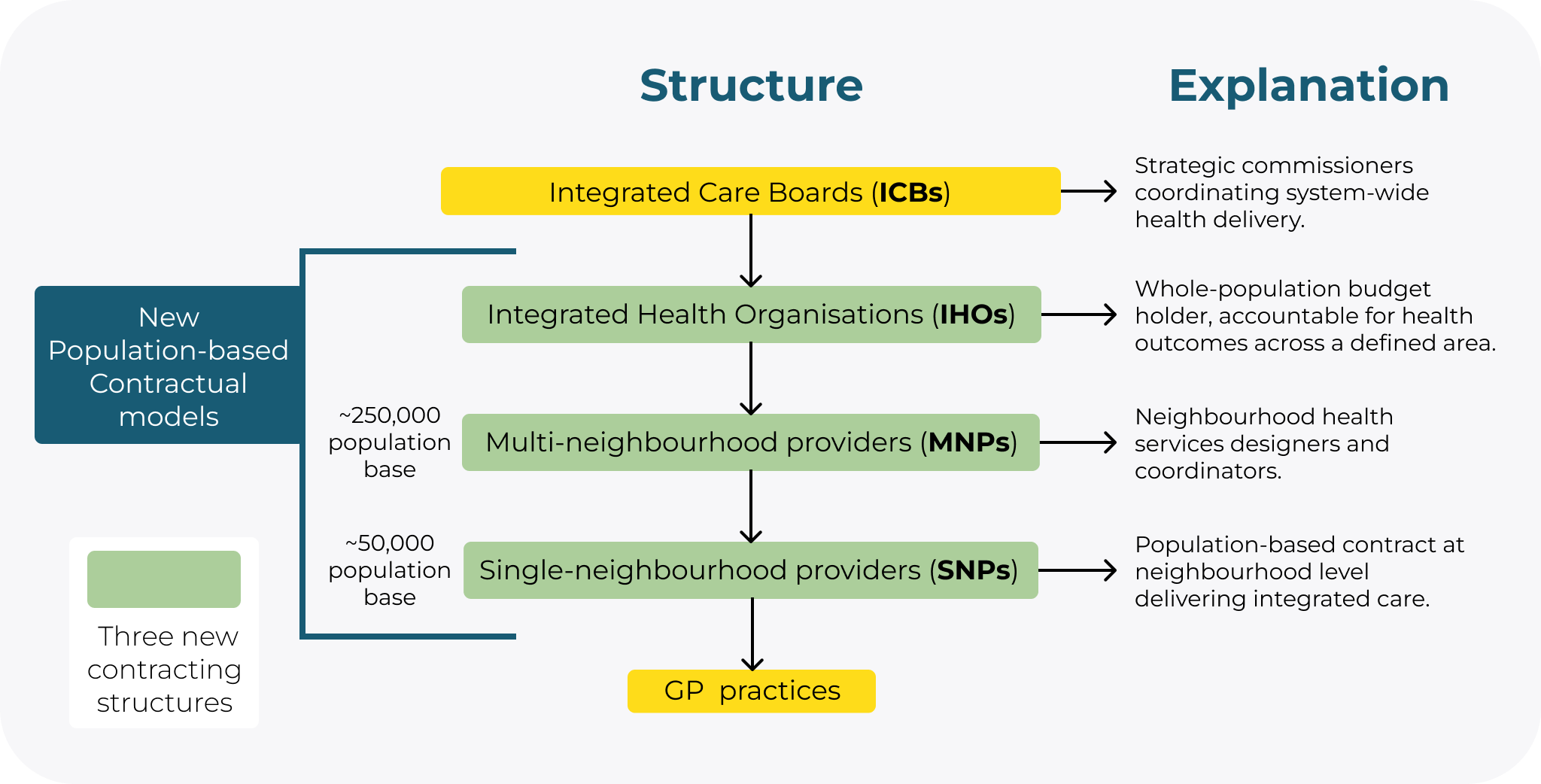
This structure signals an important shift in the role of ICBs. Rather than directly managing delivery, ICBs would move toward a more strategic system leadership and commissioning role, while Integrated Health Organisations (IHOs) take on greater responsibility for population-level integration, neighbourhood-level coordination and delegated commissioning functions, creating a model where decision-making and service design sit closer to local communities. In practice, an IHO will not be a new statutory organisation but a new integrated delivery model. This brings resource allocation and decision-making closer to the communities being served.
Beyond the operating model itself, the NHF signals three broader shifts:
1️⃣. A shift of responsibility to local systems. The model places greater emphasis on collaboration with voluntary, community, faith and social enterprise organisations (VCFSE), community partners and Health and Wellbeing Boards (HWBs), recognising that improving population health extends beyond the NHS alone.
2️⃣. A shift from crisis-led, hospital care toward proactive service delivery. This reinforces the long-discussed “left shift” toward earlier intervention closer to people’s homes and communities.
3️⃣. A shift towards rewarding measurable health improvements, moving from payment per activity (such as a hypertension test) to payment for measurable health improvement (such as a reduction in hypertension rates). This creates stronger incentives for cross-sector collaboration around shared outcomes.
The goals, contractual changes and directional shifts are welcome. The NHF goes beyond redefining contracts and feels like a cultural move towards collaboration and integration. Implemented well, this will create a real space for patients, staff and integrated teams to work together in ways the NHS has not previously been structured to do so.
The NHF is highly ambitious and proposes significant changes to the way healthcare is currently delivered, presenting a number of opportunities for the sector, and the country as a whole:
The NHS has long grappled with siloed working, where teams triage and pass patients along a pathway, with limited continuity or connection between them.
The NHF encourages health professionals from different disciplines to collaborate and get to know each other. This is not through the usual referral pathways and handoffs, but through organic and repeated contact in shared Neighbourhood Health Centres (NHC). The NHF represents an attempt to answer both the problem of siloed working as a cultural issue as well as a physical one. This is further demonstrated in the design and performance specification for NHCs.
Consider a GP seeing a patient in a mental health crisis. In the current model, the next step is a referral, often with long waits and little clarity about who holds responsibility in the meantime. In an NHC, co-located teams build working relationships through regular interaction, making a genuinely collaborative response far more likely.
In the NHC model, integrated teams share physical space, patient records and hold multi-disciplinary meetings, meaning professionals from different organisations discuss the same patient together, rather than receiving referrals in sequence. Shared accountability and knowledge replaces handoffs.
At their best, co-located and operationally integrated teams allow for collaboration to thrive and they encourage the ‘left shift’ to materialise.
However, this collaboration doesn’t just happen from sitting people next to each other. There are a number of thorny challenges to overcome in the meantime: how to share data, navigate capacity and where to invest the next pound in the various organisations represented around the table.
Under the new Framework, ICBs move into a more strategic commissioning role with IHOs sitting underneath as a population-level delivery and budget-holding vehicle. This is a move towards a localised and flexible approach where SNPs and MNPs are focused on local population needs.
The NHF also increases the strategic importance of HWBs, particularly as neighbourhood geographies begin to take shape. In many areas, HWBs are becoming increasingly influential in defining local priorities, shaping population health strategies and connecting NHS delivery more closely with wider community and local authority insight.
These new structures promote flexibility and localisation and are grounded in the idea that local communities know best.
Take HWBs for example: through ward profiles, Joint Strategic Need Assessments (JSNAs) and local knowledge they know the employment patterns, housing data, local demographic differences, key pressures and importantly, they know the local community groups and VCSFE’s. This places them in a strong position to lead local, neighbourhood health delivery. Ultimately, the needs of Clacton are different to the needs of Clapham and the NHF offers a model where local knowledge is embedded in decision making.
The challenge of this comes in supporting organisational relationships across the NHF: how much time is afforded for outcomes to come to life, how much patience, trust and empathy is extended across the Integrated Neighbourhood Team (INT)? Going forward, it is important to consider what happens when local knowledge from different perspectives contradict each other or don’t align with strategic vision.
The NHF creates conditions for more preventative care in three ways:
Collaboration, data infrastructure and financial incentives all need to work together for neighbourhood health to succeed in practice.
To put this in context: with a shift to prevention, the NHF puts emphasis on what happens before the patient reaches the door. Patients may not be known to general practice when they are outside their four walls, but they are known to their communities - to a housing officer, a community mental health charity, a volunteer group. The opportunity is to better connect these community touchpoints with integrated healthcare teams, creating a system capable of identifying and intervening earlier than traditional healthcare structures have typically managed.
The opportunities are real for the NHF, but only if we can overcome some of the practical barriers for delivery. Below we explore three key challenges that need to be addressed in order to make these major structural and cultural changes happen.
The ambition of neighbourhood health relies on multidisciplinary teams working across organisational boundaries, but this raises the question about whether the infrastructure needed to enable that integration is fully developed. Data is central to this challenge. Without the ability to securely share information, coordinate care pathways and build a shared understanding of patient need across organisations, integrated teams risk remaining structurally connected but operationally fragmented.
Regionally, as well, there may be challenges. For London, there is strong groundwork for data sharing. Through OneLondon’s SDE and London Care Record, it will be easier to integrate and share information between teams, with 90% of GP practices having data flow to the SDE. However, some regions have less developed data infrastructure and their neighbourhoods will have less ability to: identify priority groups, share patient data and map intervention outcomes. The risk here is that delivery of neighbourhood teams will vary nationally, meaning care will not be based not on local need but more on the capability of local infrastructure.
Ultimately, if data sharing infrastructure is not ironed out, traditional siloed pathways could carry on or informal communication pathways could be used to bridge the gap. A return to traditional pathways risks not fully utilising the opportunity neighbourhood health presents and informal data sharing could create further failure demand and fragmented patient care. The vision is integration. The risk is how long it will take to materialise and what happens in the interim.
It is worth noting that data sharing in the NHS is not without risk. Information governance, patient consent and cybersecurity are legitimate and serious considerations that need to be accounted for. The ambition for greater data sharing across neighbourhood teams must be matched by equally serious investment in the safeguards that make it trustworthy.
One of the more difficult questions within neighbourhood health is where responsibility for a patient ultimately sits within an integrated system. In practice, healthcare systems under pressure often develop a tendency to move patients between services based on capacity, thresholds or organisational remit. This is rarely about a lack of care or commitment from staff. More often, it reflects the operational realities of stretched systems.
The challenge for neighbourhood health is whether introducing more integrated and multidisciplinary teams genuinely simplifies accountability for patients, or whether it risks adding further complexity into an already fragmented landscape.
A patient may be supported by professionals across primary care, community services, local authorities, specialist trusts and VCFSE organisations. While the intention is more joined-up care, the question of who is ultimately responsible for coordinating support and managing risk can become less clear. Referrals may still face long waiting times, teams may still be operating under significant capacity pressures, and responsibility can become blurred.
This is particularly relevant because neighbourhood health extends beyond traditional NHS structures. Integrated teams may include social workers accountable to local authorities, nurses working within primary care and community organisations operating under entirely different governance arrangements. These organisations bring different cultures, priorities, funding models and risk thresholds into the same delivery environment.
All of this highlights the need for clearer approaches to shared accountability and clinical risk management. The NHS has tackled versions of this challenge before through mechanisms such as Shared Care Agreements between primary and secondary care. While imperfect, they represent a practical attempt to formalise responsibility across organisational boundaries. Neighbourhood health is likely to require similar operational clarity if integrated teams are to function effectively in practice.
Like any large-scale transformation programme, neighbourhood health will depend as much on effective change management as it does on structural reform. It requires organisations with different priorities, governance structures and ways of working to align around shared outcomes over a sustained period of time.
That will not be straightforward. ICBs may set strategic direction, but delivery sits across GPs, community trusts, local authorities and VCFSE organisations, each operating within different financial, operational and regulatory environments. Building effective neighbourhood teams will require careful coordination, strong local leadership and a willingness to learn from previous attempts at integrated working across health and care.
Effective multi-disciplinary teams are built on long-term relationships and ongoing commitment into working together. Where projects are restricted to short budget cycles or limited funding, often due to external processes or pressures, lasting change is hard to embed change because teams might not have the time to work effectively.
The risk is not that the NHF lacks ambition, but that the ambition does not match the change management processes that facilitate transformation. In reality, integrated working requires sustained investment in leadership, culture, operational coordination and workforce development if the vision of neighbourhood health is to translate into day-to-day delivery.
With the major structural changes proposed in NHS delivery, the clearest way to see how it can be made happen is by looking at where previous initiatives have been successful and why. The most successful examples of transformation have tended to focus not just on structural redesign, but also on investing in the operational and cultural conditions that allow integration to work day-to-day.
The Wigan Deal
The Wigan Deal is one of the clearest examples of long-term public service transformation built around integration, collaboration and community-based delivery. Rather than focusing solely on structural reform, the programme invested heavily in culture, leadership and relationship-building across services.
A key part of this was the BeWigan Experience, which helped staff understand the wider mission behind the transformation and how different organisations and teams contributed to shared outcomes. This led to shared values and a common understanding of the mission across the council, with staff alignment on what the deal means for the council reaching 87.8%. Wigan also introduced multi-agency service delivery footprints designed around local population needs of 30,000-50,000 residents, creating more consistent collaboration between services and clearer shared responsibility across teams.
The lesson for neighbourhood health is clear: integrated working requires sustained investment in culture, relationships and operational coordination over time.
London’s Neighbourhood Health Infrastructure
London provides an example of how investment in enabling infrastructure can support integrated care at scale. Through initiatives such as the London Care Record and wider Shared Data Environment (SDE) infrastructure, the region has built stronger foundations for data sharing and coordinated care across organisations.
Alongside digital infrastructure, London ICBs have also committed over £100 million from 2026/27 toward neighbourhood health delivery, including funding focused on behavioural and cultural change as well as estates and operational models. This reflects an understanding that successful integration depends not only on organisational redesign, but on supporting teams to work differently in practice.
The London example highlights the importance of pairing structural reform with investment in the underlying systems, relationships and capabilities needed to make integrated care operationally viable.
Thames Freeport’s Health Innovation Programme
Across Barking & Dagenham, Havering and Thurrock, spanning both North East London and Mid & South Essex ICBs/Essex ICB, PUBLIC has been working with Thames Freeport on piloting what proactive, neighbourhood-based healthcare can look like in practice.
Its programmes bring together NHS organisations, local authorities, pharmacies, VCFSEs and technology providers to deliver preventative care directly to underserved communities. In the NHF, it outlines the need for care as accessible to priority groups as close to their home as possible. This programme is a type of place-based collaboration the NHF asks for. It shows how integrated care models can work in practice across organisational boundaries.
This work demonstrates how neighbourhood-style healthcare transformation is already beginning to emerge through locally led experimentation, cross-sector collaboration and sustained investment in the operational foundations required for integrated care. It translates the ambitions of the NHF into practice and outlines what it requires at ground level: local leadership, cross-sector partnership, sustained investment and a willingness to test how integrated models can work in reality.
It brings great new opportunities and provides the NHS with delivery guidance to make the ‘left shift’ possible. It is not without its challenges, like with any transformation.
Through careful change management, led culturally from the top, with sustained decisions (with support from all levels of management) that invest in creating the conditions for collaboration rather than assuming they happen naturally, neighbourhood teams can operationally deliver and achieve the ambitions set out in the Neighbourhood Health Framework.
If you would like to discuss this further reach out to florence.mayo@public.io
.png)
Great ideas often fail not because of technology, but because they're not communicated effectively. Discover how a breakthrough data tool almost failed, until its creator learned to communicate its value effectively.

The Strategic Defence Review aims to modernise the MOD's relationship with industry and streamline technology adoption. This article outlines five critical shifts, including empowering frontline personnel and evolving internal ways of working, to turn this vision into reality.
.png)
Ryan Shea, Managing Director of PUBLIC, discusses the challenges and opportunities facing the new government.

Discover our latest interview with Elina Lam-Gall, the driving force behind PUBLIC’s efforts in transforming how government officials learn and adapt to the digital world.

As it becomes more of an essential requirement for day to day functioning, data proficiency can be seen as a pinnacle part of workforce transformation as it encourages companies to lean more into data driven decision making. Should this become a priority area?

In order to achieve a truly data-driven public sector we must embed a 'data culture' across all departments to complement data skills training.

To meet unforeseen threats with agile solutions, maintaining a digitally-literate workforce is essential in modern defence, but can we achieve this through training and culture alone?

PUBLIC, together with Daintta, is arming local councils with the learning tools they need to improve supply chain resilience and protect themselves against a growing number of cyber security threats.



