

Dig a little deeper, and the ambition is even more striking:
It’s hard to argue with these areas of focus. Equally, it’s hard not to notice how ambitious this is compared to the last decade of progress around NHS reform. However, there is a chance that this time is different. The pressures are understood, the tools are ready, and the political alignment is unusually strong:
So the ambition is right, and the moment is right. The real question is whether we can deliver it. And here’s where the NHS needs a new playbook: one that doesn’t assume reform can simply be designed in Whitehall and pushed out nationally, but instead creates disciplined ways to test, adapt and scale solutions in the messy reality of frontline care.
Even well-resourced programmes sometimes struggle to deliver expected impact. New services and care models can inadvertently increase demand or costs. NHS 111 or urgent care centres, for example, expanded access but sometimes drove more patients into hospitals rather than alleviating pressure.
The impact of innovation programmes often depends on how they are structured:
The consequence is predictable: money, time, and effort are invested, but the system sees limited returns. Inefficiencies persist, and opportunities to improve outcomes, reduce costs, or streamline care are lost. Without structured experimentation, innovation can end up reproducing the very problems it was meant to solve.
A challenge programme is a structured, problem-first approach to innovation. It starts with a question:
“How might we… transform care delivery, redesign pathways, or optimise resources?”
It mobilises a diverse set of actors - frontline staff, innovators, commissioners, and community partners - to co-create and test interventions in real-world conditions. Unlike traditional approaches, where solutions are pitched to pre-defined domains, a challenge programme embeds experimentation directly into the system. Interventions are tested, refined, and scaled based on operational evidence.
A notable example of effective practitioner-led experimentation is the NHS Test Beds Programme. By bringing together NHS organisations, technology companies, patients, and carers, the programme demonstrated how real-world pilots can test integrated digital solutions safely and effectively. Innovations were refined through iterative feedback, combining technology with pathway redesign, and generating evidence that could be scaled across the NHS. The Test Beds Programme highlights the value of embedding experimentation within operational realities, showing that collaboration between frontline staff, innovators, and commissioners can produce realisable benefit ratios relative to more traditional models.
The principle is simple: complex problems cannot be solved top-down alone. In the start-up world, where uncertainty is expected and outcomes rarely guaranteed, success comes from disciplined experimentation, rapid iteration, and evidence-based scaling. The NHS can borrow these principles to improve delivery, reduce cost, and generate sustainable impact.
Challenge programmes are time-bound, cohort-driven, and problem-first:
Even the best programmes have limits. Lessons from the NHS AI in Health and Care Award illustrate this:
These examples underline a broader truth: Structured experimentation must be complemented by careful management of uncertainty, robust governance, and planning for long-term sustainability and scale.
Across NHS innovation initiatives, four dimensions are critical to maximise impact:
While many programmes have made valuable contributions, some innovations - such as AI pilots - have shown the importance of robust governance, national coordination, and implementation support to fully realise their potential. Emphasising these dimensions can help ensure that promising solutions are effectively adopted, scaled, and sustained across the NHS.
To maximise impact, we propose a network-based challenge programme that embeds experimentation directly into the NHS system while ensuring learning is transferable and interventions are scalable.
Core Components:
Implementation Phases:
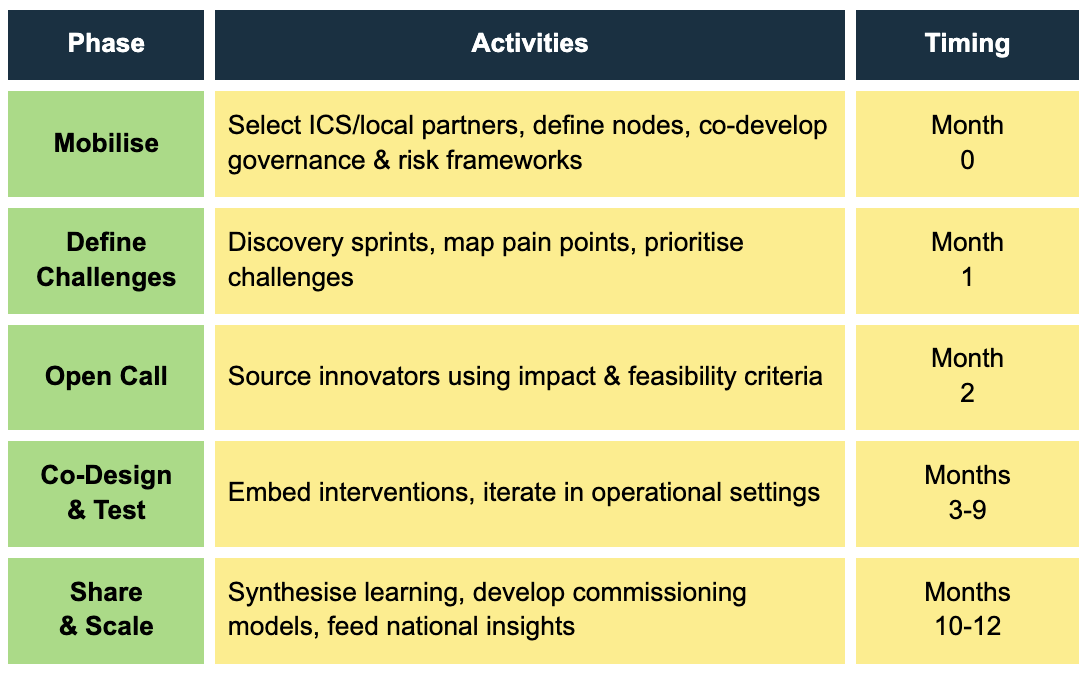
A Primary Care Network, working with local GP practices, deploys this Challenge Programme model to improve hypertension management:
To ensure safety, effectiveness, and scalability, programmes must address:
The NHS 10 Year Plan is a thoughtful call to action that is focused on the right problems. To help it succeed, we believe calculated risk taking and experimentation alongside robust measurement, is how the NHS can deliver on this Plan. Doing this in a place-based way that accepts the nuance and complexity of the challenges to be solved, bringing clinicians, local governments, third sector, entrepreneurs, and patients along helps ensure the right feedback loops and improve the chances for success.
Special thanks to the following contributors:
Tara Donnelly (Founder of Digital Care and former Chief Digital Officer of NHS England)
Malte Gerhold (Director of Innovation and Improvement of the Health Foundation and Executive Director of the Care Quality Commission)

Announcing the eleven finalist consortium selected for Round 6 of the PropTech Innovation Fund, as part of MHCLG's Dgital Planning Programme with PUBLIC.
.png)
Explore how Thames Freeport is redefining economic zones by launching AI-driven mobile health clinics and pioneering digital frameworks to directly tackle local NHS backlogs and boost workforce health.

In the latest episode of Talking GovTech, PUBLIC’s video interview series, Florrie Mayo, Manager of Innovation Programmes, speaks to Tom White, Head of Innovation and Skills at Thames Freeport.

Explore how hackathons can be a powerful tool for any government team looking to leverage key datasets they have at their fingertips.
The Inside GovTech Spotlight, shining a light on exciting companies that are making a difference to public services through technology; to share their success stories and advice, offer civil servants new ideas on how to tackle complex problems, and encourage other innovators to consider their solution’s potential to address crucial public sector challenges.

The Inside GovTech Spotlight, shining a light on exciting companies that are making a difference to public services through technology; to share their success stories and advice, offer civil servants new ideas on how to tackle complex problems, and encourage other innovators to consider their solution’s potential to address crucial public sector challenges.

How has the GovTech market evolved and how should the UK government react?
.png)
PUBLIC and Digital Care are joining Challenge Works to support five finalist teams in developing cutting-edge tech solutions to help those living with early-stage dementia lead more independent lives.

Explore the pivotal role of social well-being and citizen engagement in shaping smart cities with GovTech Connect 2024 Boot Camps, where startups lead the charge towards inclusive, sustainable urban development.

Explore the transformative potential of the next round of GovTech Connect 2024 Boot Camps, where startups will converge to pioneer smart solutions for sustainable, innovative cities,
.png)
PUBLIC and Amazon Web Services (AWS) team up to host AI in the Public Sector Showcase to drive the adoption of AI-powered solutions to improve government services.

PUBLIC's Head of Communications, Natasha Wren, sits down with Chiara Carlini, our Head of Open Innovation Programmes at PUBLIC, to explore her journey and insights into the innovation ecosystem across Europe.




